Recurrent Ankle Sprains?
Why You Shouldn’t Delay Treatment!
One of the most common sports injuries that will often go untreated is the ankle sprain. Most of us have experience with an ankle sprain, especially in sports that involve quick changes of direction, landing and jumping such as netball, basketball and football. However, the ankle sprain is not only a common injury experienced by athletes, it also affects many people that do not participate in sports and can easily occur by walking on uneven surfaces or by accidentally stepping into a pothole. Each year, around 230,000(1) Australians seek help for an ankle sprain signifying the high prevalence of this common injury.
However, most people do not fully rehabilitate the ankle which leads to recurrent ankle sprains and in some instances, long standing ankle pain and instability.
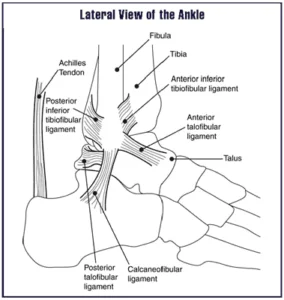 Let’s have a look at the anatomy of the ankle. On the outside of the ankle there are three major ligaments: the anterior talofibular ligament (ATFL), the posterior talofibular ligament (PTFL), and the calcaneofibular ligament (CFL). The common ankle sprain usually involves injury to the ATFL and CFL. These sprains occur when the ankle “rolls” inwards and takes the ankle joint beyond the ligament’s length which can lead to a sprain. The degree of ligament tear is classified as a grade of ankle sprain. These grades range from a grade one which is a small, minor tear, to a grade three which is a total rupture of the ligament. Ligaments are very tough and, in some cases, shear off a chip of bone rather than tear themselves. This is known as an avulsion fracture.
Let’s have a look at the anatomy of the ankle. On the outside of the ankle there are three major ligaments: the anterior talofibular ligament (ATFL), the posterior talofibular ligament (PTFL), and the calcaneofibular ligament (CFL). The common ankle sprain usually involves injury to the ATFL and CFL. These sprains occur when the ankle “rolls” inwards and takes the ankle joint beyond the ligament’s length which can lead to a sprain. The degree of ligament tear is classified as a grade of ankle sprain. These grades range from a grade one which is a small, minor tear, to a grade three which is a total rupture of the ligament. Ligaments are very tough and, in some cases, shear off a chip of bone rather than tear themselves. This is known as an avulsion fracture.Following an ankle sprain you will usually feel immediate pain around the ankle, especially when you bear weight on the injured foot. You may have heard a popping sensation or sound at the time of injury. Usually there will be a degree of swelling around the ankle in addition to bruising. You may also have restrictions in the flexibility in your ankle due to pain and swelling. It’s important to follow the R.I.C.E protocol following an ankle sprain that is; Rest, Ice, Compression and Elevation to control swelling and prevent further damage.
Diagnosing an ankle sprain is easily done by your physiotherapist. X-rays generally are not recommended for typical ankle sprains unless you are unable to walk on the injured foot or you have pain in specific locations on the ankle that indicate more severe damage has occurred(2). Receiving the proper treatment and rehabilitation is essential so that the ankle recovers, avoiding ongoing pain and most importantly: preventing re-injury.
At Peak MSK physiotherapy, we commence treatment in line with current research immediately following an ankle sprain and implement a comprehensive treatment program to effectively rehabilitate the ankle(3). Rehabilitation when the early acute pain and swelling settles, includes manual therapy techniques, taping, bracing, soft tissue massage, to enable pain-free joint movement and exercise.

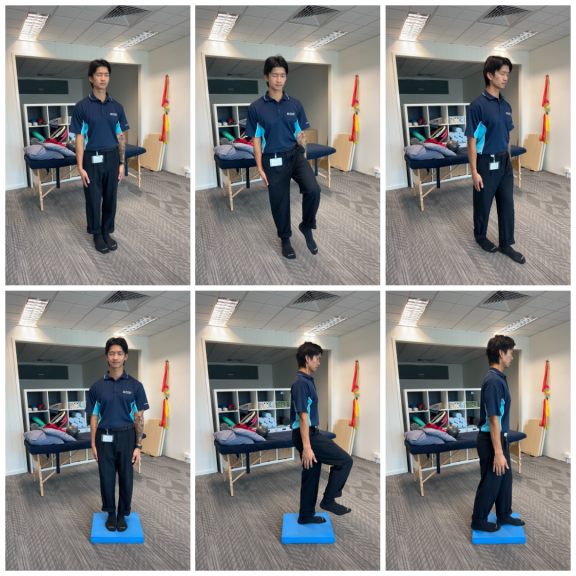
A graded rehabilitation exercise program is key to success!
The exercise program comprises of muscle strengthening, range of motion and proprioception training to get your ankle nice and strong so you can return to playing the sports you love, injury and pain free. Proprioception is related to your balance receptors and the ability to tell what your ankle is doing when you aren’t paying attention to it.
If you have any concerns regarding ankle sprains, call Peak MSK physio on 9533 5305 to book an appointment with one of our Physiotherapists. Drop us a comment below to start a conversation with our team.
References
1. Pollack A, Bayram C, Miller G. (2016). Musculoskeletal Injury in Australian General Practice: 2000 – 2015. Aust Pham Physician, 45:462-5.
2. Bachmann L, Kolb E, Koller MT, Steurer J, ter Riet G. (2003). Accuracy of Ottawa ankle rules to exclude fractures of the ankle and mid-foot: systematic review. BMJ, 326(7386):417. doi:10.1136/bmj.326.7386.417.
3. Doherty C, Bleakley C, Delahunt E, et al. (2017). Treatment and prevention of acute and recurrent ankle sprain: an overview of systematic reviews with meta-analysis. Br J Sports Med, 51:113–125.
1. Pollack A, Bayram C, Miller G. (2016). Musculoskeletal Injury in Australian General Practice: 2000 – 2015. Aust Pham Physician, 45:462-5.
2. Bachmann L, Kolb E, Koller MT, Steurer J, ter Riet G. (2003). Accuracy of Ottawa ankle rules to exclude fractures of the ankle and mid-foot: systematic review. BMJ, 326(7386):417. doi:10.1136/bmj.326.7386.417.
3. Doherty C, Bleakley C, Delahunt E, et al. (2017). Treatment and prevention of acute and recurrent ankle sprain: an overview of systematic reviews with meta-analysis. Br J Sports Med, 51:113–125.